Glossary
Root Cause Analysis
What is root cause analysis?
Root cause analysis, often shortened to RCA, is a structured way to find the underlying causes of a problem instead of stopping at the visible symptom. Teams use RCA after incidents, defects, outages, safety events, missed handoffs, customer complaints, and recurring process failures.
A useful RCA is not an explanation exercise. It identifies what must change so the same problem is less likely to happen again.
Why root cause analysis matters
Most problems announce themselves through symptoms: a late report, a broken handoff, a customer escalation, an outage, a safety near miss, or a quality defect. Removing the symptom may be enough for a one-off nuisance, but it is weak when the same failure could repeat.
Root cause analysis slows the team down just enough to ask better questions. What conditions made the problem possible? Why did existing checks miss it? Was the process unclear, the tool misconfigured, the owner missing, the training incomplete, or the workload unrealistic?
OSHA's incident-investigation guidance makes this point clearly in the safety context: investigations need to look beyond immediate causes to find systemic changes that can prevent future incidents.1 That same principle applies outside safety work too. If the fix does not change the system, the system may produce the same result again.
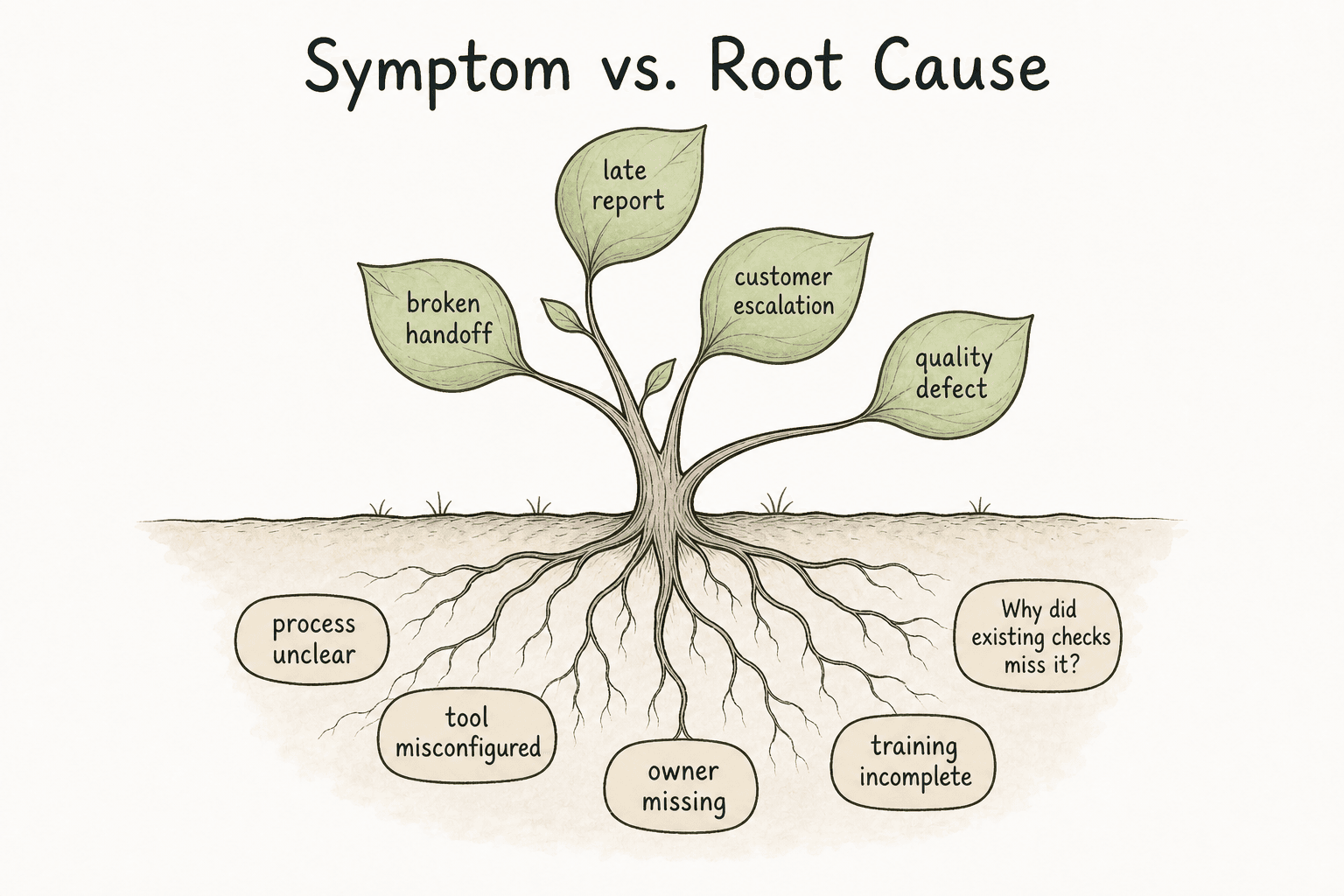
Root cause vs. symptom
A symptom is what people notice first. A root cause is the deeper condition that allowed the symptom to happen. There may be more than one root cause, and there are often contributing factors around it.
| Visible symptom | Shallow fix | Stronger RCA question |
|---|---|---|
| A checklist step was skipped | Remind the team | Why was the step easy to miss? |
| A customer got the wrong answer | Correct the one ticket | Why did the old knowledge article surface first? |
| A report was late | Ask for faster follow-up | Why was no owner assigned after handoff? |
| A service failed after deployment | Roll back the release | Why did pre-release checks miss that failure mode? |
A useful RCA does not assume one person forgot one thing. Google SRE's blameless postmortem guidance frames postmortems as learning tools that identify contributing causes without indicting individuals or teams.2 RCA looks at the design of the work around the person: documentation, controls, tooling, communication, ownership, training, incentives, and review cadence.

How root cause analysis works
A simple RCA workflow usually looks like this:
- Define the problem in concrete terms.
- Gather evidence and build a short timeline.
- Identify immediate causes and contributing factors.
- Ask why those causes existed.
- Validate likely root causes against the evidence.
- Choose corrective actions tied to those causes.
- Assign owners, due dates, and a verification plan.
- Update documentation, training, controls, or workflows.
The strongest step is validation. A cause should be more than a plausible story. It should fit the timeline, evidence, and operating context. If the team cannot show why a cause is likely, it may be guessing.
A practical RCA example
Imagine a support team repeatedly misses escalations for urgent billing issues. The symptom is missed escalations. A shallow fix is to remind agents to follow the escalation policy.
A stronger RCA might find that the billing escalation path appears in three different places, the current version is not obvious, and the support form does not require agents to tag billing severity. The root cause is not merely attention. It is a documentation and workflow design problem.
A better corrective action would connect the updated escalation path to the support form, archive old guidance, add a severity prompt, and assign an owner to review billing escalation instructions after policy changes.
Common RCA tools
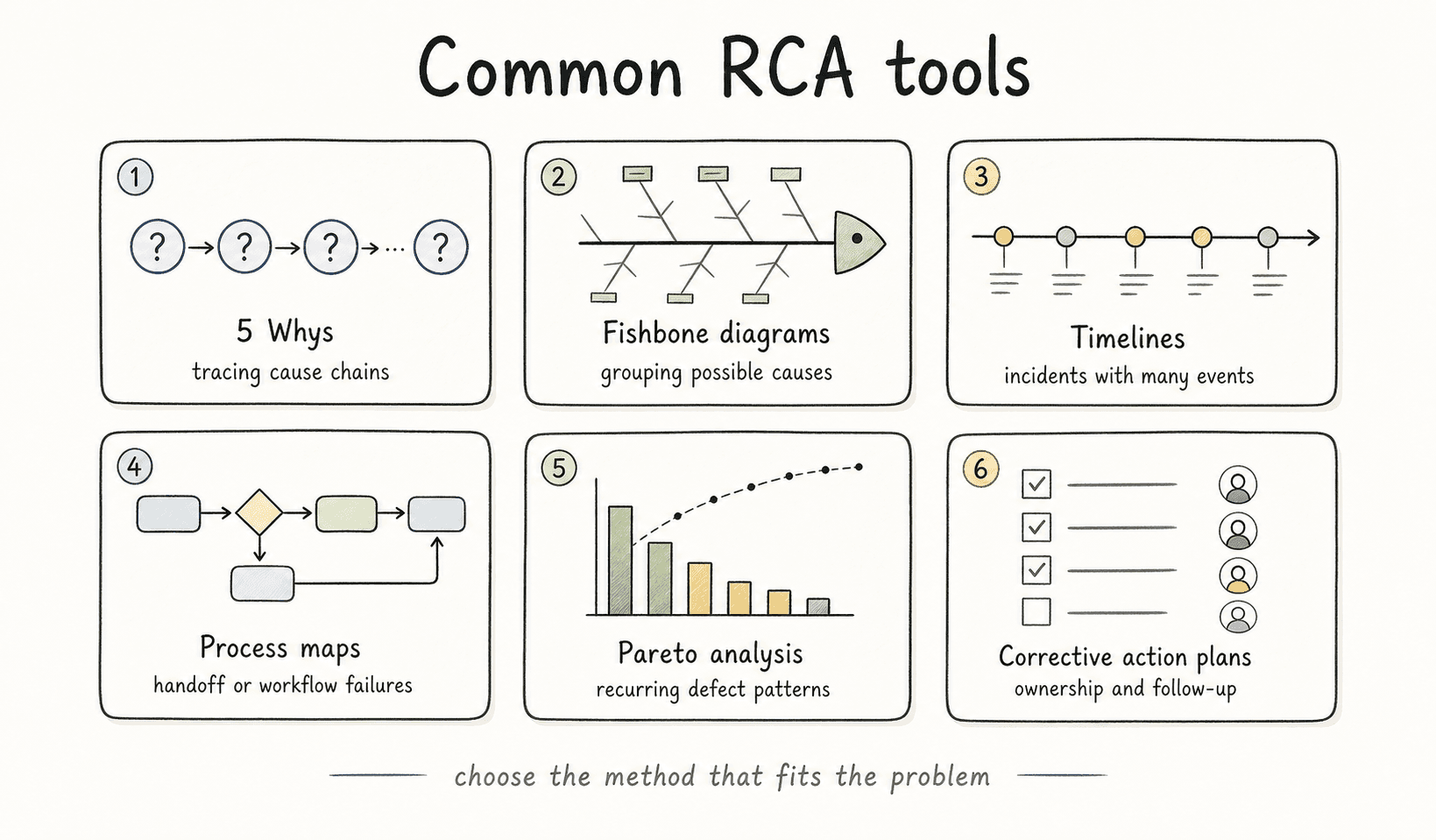
Root cause analysis is a discipline, not one required tool. Teams should choose the method that fits the problem.
Common tools include:
- 5 Whys for tracing cause chains
- Fishbone diagrams for grouping possible causes
- Timelines for incidents with many events
- Process maps for handoff or workflow failures
- Pareto analysis for recurring defect patterns
- Corrective action plans for ownership and follow-up
The tool should clarify the work, not perform theater. CMS root cause analysis guidance names techniques such as 5 Whys, flowcharting, and fishbone diagrams, but ties them back to identifying root causes and corrective action plans.3 If a fishbone diagram creates ten categories but no better corrective action, it has not helped.
What to document
RCA documentation should make the reasoning visible. Someone reading it later should understand what happened, what evidence was considered, what was ruled out, and why the chosen actions match the cause.
Capture:
- Problem statement, scope, and impact
- Timeline and evidence reviewed
- Immediate causes and contributing factors
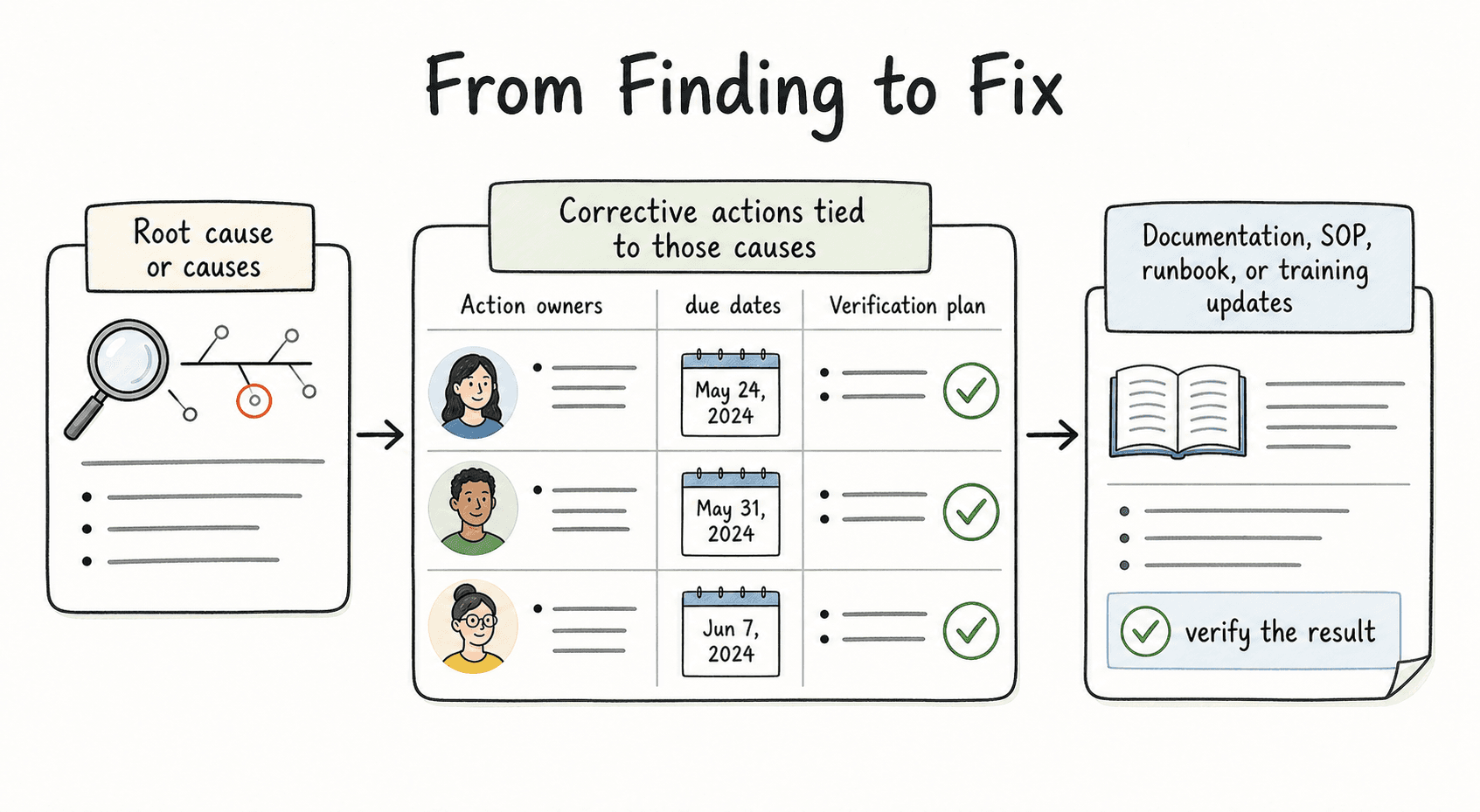
- Root cause or causes
- Corrective actions tied to those causes
- Action owners and due dates
- Verification plan
- Documentation, SOP, runbook, or training updates
The verification plan is often where RCA becomes real. NIST incident response guidance connects lessons learned and root cause analysis to improved risk management and future readiness, not just post-incident reporting.4 If nobody checks whether the corrective action worked, the organization has written a report, not improved the process.
Common mistakes
Turning RCA into blame. If people feel the goal is to find a culprit, they will defend themselves instead of surfacing the conditions that made failure likely.
Stopping at "human error." Human error may describe what happened, but it rarely explains why the work system made that error possible or hard to catch.
Choosing weak corrective actions. Reminders, retraining, and policy updates may help, but durable fixes often involve clearer ownership, better workflow controls, simpler tools, updated documentation, or built-in checks.
Documentation takeaway
Root cause analysis turns a problem into a documented learning loop: define the issue, investigate the evidence, identify causes, assign corrective action, and verify the result.
When the cause points to missing instructions, unclear handoffs, outdated runbooks, or tribal knowledge, the documentation update is part of the fix, not a side note.
How Trails helps
Trails helps teams capture and maintain repeatable process documentation. After RCA, Trails can help document the improved workflow, create updated SOPs or runbooks, and make the new process easier to train and follow.
- Retrospective
- Continuous improvement
- Process improvement
- Standard operating procedure
- Runbook
- 5 Whys
- Corrective action
- Fishbone diagram
Sources
- 1
Occupational Safety and Health Administration. Incident Investigation. OSHA. www.osha.gov/incident-investigation. Accessed July 9, 2026.
- 2
Google SRE. Blameless Postmortem Culture. Google. sre.google/sre-book/postmortem-culture/. Accessed July 9, 2026.
- 3
Centers for Medicare & Medicaid Services. Guidance for Performing Root Cause Analysis with PIPs. CMS. www.cms.gov/medicare/provider-enrollment-and-certification/qapi/downloads/guidanceforrca.pdf. Accessed July 9, 2026.
- 4
National Institute of Standards and Technology. Incident Response Recommendations and Considerations. NIST, 2025. nvlpubs.nist.gov/nistpubs/specialpublications/nist.sp.800-61r3.pdf. Accessed July 9, 2026.